Comprehensive Pharmacological, Clinical, and Regulatory Analysis of the KLIKGLOW 70mg Multi-Peptide Complex (GHK-Cu, BPC-157, TB-500)
The Paradigm Shift in Combinatorial Peptide Therapeutics The modern landscape of regenerative medicine, systemic anti-aging aesthetics, and musculoskeletal sports recovery has undergone a radical transformation over the past decade. Historically, the application of synthetic peptide therapeutics was characterized by monotherapy, wherein single bioactive amino acid chains were administered to target highly specific biological bottlenecks, such as isolated growth hormone deficiency or localized wound healing. However, contemporary clinical practice, operating alongside a highly engaged and risk-tolerant biohacking community, has increasingly pivoted toward combinatorial peptide formulations. These advanced formulations, colloquially referred to as “stacks” within performance-enhancement lexicons, are engineered to target multiple physiological pathways simultaneously, thereby creating a synergistic environment that theoretically accelerates cellular repair and systemic rejuvenation beyond the capabilities of any single compound.
Among the most prominent and heavily scrutinized of these advanced combinations is the KLIKGLOW 70mg peptide complex, frequently marketed by vendors and wellness clinics under variations of the name “Glow Blend” or “Pure Glow Fusion”. Supplied primarily as a lyophilized powder in sealed laboratory vials, or administered via intravenous (IV) and subcutaneous routes in concierge medical settings, the KLIKGLOW 70mg formulation represents a highly specific stoichiometric aggregation of three distinct bioactive peptides. The formulation specifically combines 50mg of GHK-Cu (Copper Tripeptide-1), 10mg of BPC-157 (Body Protection Compound), and 10mg of TB-500 (a synthetic Thymosin Beta-4 fragment), yielding a total molecular peptide weight of 70mg per unit.
Officially, the manufacturers and distributors of the KLIKGLOW complex explicitly market the product as a multi-compound research preparation intended strictly for in-vitro, analytical, and laboratory evaluation. Distributors state that the compound is designed to support controlled scientific investigations into peptide stability, structural characteristics, and molecular behavior in multi-compound experimental systems, firmly disclaiming human or veterinary use.
Despite these stringent “research-only” disclaimers—which serve primarily as a legal shield to circumvent pharmaceutical regulatory frameworks—the formulation has been widely adopted for off-label human use. Wellness clinics, telehealth providers, and independent consumers utilize the blend to accelerate deep tissue repair, modulate chronic systemic inflammation, stimulate profound collagen synthesis, and initiate systemic rejuvenation from the cellular level outward.
This exhaustive analytical report investigates the complex pharmacological mechanisms of the KLIKGLOW 70mg components, evaluating their theoretical synergy. Furthermore, the report meticulously tracks the current status of human clinical testing, analyzes real-world observational data derived from social media ethnography, and decodes the highly volatile 2026 regulatory landscape governing these unapproved synthetic therapeutics across global jurisdictions.
Product Architecture and Commercial Distribution
To fully contextualize the clinical relevance of the KLIKGLOW 70mg complex, one must examine its commercial architecture and the dichotomy between its intended chemical classification and its real-world application. The formulation utilizes a specific mass ratio of 5:1:1, combining 50mg of the copper-binding tripeptide GHK-Cu, 10mg of the pentadecapeptide BPC-157, and 10mg of the heptapeptide TB-500. This specific ratio is not arbitrary; it is designed to provide a massive foundational dose of genomic and structural matrix support (via GHK-Cu) while delivering potent, equipotent clinical doses of acute inflammatory modulators and cellular migration catalysts (via BPC-157 and TB-500).
The Distribution Dichotomy: Gray Market vs. Clinical Application
The distribution of the KLIKGLOW complex is bifurcated into two distinct operational models: direct-to-consumer gray market research channels and concierge medical administration.
In the direct-to-consumer market, vendors such as “The Secret Beauty Store” retail the Glow Blend 70mg as a research-grade, multi-peptide complex priced at approximately £62.50 per vial. These products are supplied as lyophilized (freeze-dried) powders in tamper-evident vials, requiring the end-user to reconstitute the peptides with bacteriostatic water for subcutaneous injection. The marketing language accompanying these products is strictly sterile, emphasizing that each batch undergoes internal analytical verification for purity to ensure suitability for regulated laboratory environments.
Conversely, the formulation is actively utilized in human subjects within the burgeoning concierge medical and intravenous (IV) therapy sectors. Clinics such as “IVs in the Keys” and various telehealth weight-loss and wellness centers market the “Glow Stack” directly to patients for approximately $350 per treatment session. In these settings, the formulation is often administered as an IV therapy infusion or a guided subcutaneous protocol (often structured as a 6- or 12-week regimen, injecting five days a week). Clinical marketing materials shed the “research-only” pretense, explicitly touting the blend as a premium aesthetic and regenerative powerhouse that targets muscles, tendons, skin, fascia, and blood vessels to reverse the signs of aging and injury.
Sourcing and Manufacturing Obfuscation
The supply chain underpinning the KLIKGLOW formulation is notoriously opaque, a defining characteristic of the modern synthetic peptide market. Various distributors claim that the peptides are sourced from “APEX Pharma,” asserting that the compounds are synthesized in state-of-the-art biotech facilities featuring GMP-aligned development practices and rigorous analytical purity verification.
Research into corporate pharmaceutical registries indicates that an entity named Apex Pharma is a large, legitimate pharmaceutical manufacturer headquartered in Chennai, India, with advanced WHO Maturity Level 3 facilities operating in Egypt. However, the digital peptide market frequently utilizes corporate nomenclature mimicry to establish unwarranted legitimacy. Several entities operating under variations of the name (e.g., Apex Peptide Supply, APEX Peptides) exist within the United States as digital storefronts distributing unverified research chemicals.
Some product formats, such as the “KLIKGLOW 70mg pre-filled research device” (a peptide injector pen), attempt to mimic the delivery systems of legitimate pharmaceutical biologics, blurring the line between clinical medicine and unregulated biohacking. Because these products are categorized as research chemicals, they fundamentally bypass the strict sterility, endotoxin, and immunogenicity testing protocols mandated for FDA-approved pharmaceutical injectables, introducing severe variables regarding product purity and safety.
Pharmacodynamics and Molecular Mechanisms of Action
To comprehend the profound physiological shifts reported by users of the KLIKGLOW complex, it is necessary to deconstruct the molecular and genomic mechanisms of its three constituent peptides. While each compound targets a distinct phase of the cellular repair cycle, their integrated function represents a highly sophisticated approach to biological remodeling.
BPC-157: Angiogenesis and Cytoprotective Modulation
Body Protection Compound-157 (BPC-157), occasionally designated by its developmental codes Bepecin or PL 14736, is a synthetic, 15-amino-acid pentadecapeptide. The sequence is derived from a naturally occurring, high-molecular-weight protective protein found in human gastric juice. Originally investigated by researchers for its profound cytoprotective effects on the gastrointestinal mucosa—specifically in the healing of gastric ulcers and inflammatory bowel disease—the therapeutic potential of BPC-157 has since expanded dramatically into the realms of severe musculoskeletal repair, soft tissue regeneration, and advanced neuroprotection.
The primary, and perhaps most clinically significant, mechanism of action for BPC-157 revolves around the vigorous promotion of targeted angiogenesis—the complex physiological process through which new microvascular networks form from pre-existing blood vessels. BPC-157 achieves this pro-angiogenic state by significantly upregulating the cellular expression of Vascular Endothelial Growth Factor Receptor 2 (VEGFR2). By activating the highly specific VEGFR2-Akt-eNOS signaling pathway, BPC-157 enhances endothelial cell proliferation and survival. This enhanced microvascular integrity fundamentally alters the local biological environment, ensuring an exponentially higher delivery rate of oxygen, growth factors, and critical nutrients to tissues that are notoriously avascular or poorly vascularized, such as dense tendons, ligaments, and deep cartilage matrices, thereby dramatically accelerating their biological repair timelines.
Furthermore, BPC-157 operates on a profound intracellular level by stimulating the FAK-paxillin pathway. Focal adhesion kinase (FAK) and paxillin are instrumental mechanotransduction proteins that regulate how cells attach to the extracellular matrix and migrate across it. By increasing the phosphorylation and activation of FAK and paxillin within tendon fibroblast cells, BPC-157 drives the rapid migration and proliferation of fibroblasts directly into acute injury sites, laying down new tissue scaffolding at an accelerated rate.
Beyond musculoskeletal healing, BPC-157 exerts profound, yet poorly understood, modulatory effects on the central nervous system, heavily influencing the gut-brain axis. Complex pharmacological animal models suggest that the peptide interacts intricately with multiple neurotransmitter networks, including the dopaminergic, serotonergic, GABAergic, and opioid systems. In controlled rat models, BPC-157 has demonstrated the capacity to completely counteract amphetamine-induced toxicity, reverse neuroleptic-induced catalepsy (often triggered by haloperidol), and mitigate the life-threatening cascade of serotonin syndrome induced by excessive serotonin precursor availability. Additional highly specific studies involving ketamine-induced schizophrenia-like symptoms in rats demonstrated that BPC-157 effectively counteracted severe cognitive dysfunction, profound social withdrawal, and chemically induced anhedonia. The peptide achieves these complex neurological stabilizations largely through intricate, bidirectional interactions with the nitric oxide (NO) system, dynamically responding to both NO-system blockade (via L-NAME administration) and NO-system over-stimulation (via L-arginine administration) to restore neurological homeostasis.
TB-500: The Catalyst for Directed Cellular Migration
TB-500 is a synthetic heptapeptide, consisting of a highly specific seven-amino-acid sequence (Ac-LKKTETQ). It is vital to note that TB-500 is not a naturally occurring compound; rather, it represents the synthesized active binding fragment of a much larger, naturally occurring 43-amino-acid protein known as Thymosin Beta-4 (Tβ4). In human physiology, the full-length Tβ4 protein is endogenously upregulated and released in massive quantities following severe tissue injury, playing an absolutely critical role in controlling localized inflammation, mitigating cellular death, and facilitating structural repair.
The synthetic TB-500 fragment seeks to isolate and replicate the primary biological activity of its parent molecule, specifically regarding the regulation of actin. Actin is an abundant cellular protein that forms the microfilaments of the cytoskeleton, dictating a cell’s shape and its ability to move. TB-500 functions as an aggressive actin-sequestering agent; by physically binding to globular actin (G-actin), the peptide prevents premature polymerization into filamentous actin (F-actin), thereby maintaining a pool of ready-to-use actin monomers. This complex mechanism of cytoskeletal organization dramatically enhances cellular mobility.
By upregulating actin dynamics, TB-500 allows vital repair cells, including progenitor cells, endothelial cells, and fibroblasts, to migrate rapidly and efficiently across the damaged extracellular matrix directly to the site of an injury. In preclinical rodent models, this directed cellular migration translates to profoundly accelerated wound healing, significantly decreased tissue fibrosis (scar tissue formation), and the robust architectural recovery of skeletal muscle and tendon tissue following severe crush injuries or lacerations.
Like BPC-157, TB-500 also exhibits potent pro-angiogenic properties, stimulating the formation of new blood vessels to nourish regenerating tissue, making the two peptides highly complementary in their repair mechanisms. Recent advancements in peptide engineering have even explored the creation of tandem thymosin beta-4 (tTB4) molecules—fusing two monomers to create dual G-actin binding domains—which have shown superior bioactivity in treating severe corneal wounds, highlighting the immense pharmacological potential of this specific amino acid sequence.
GHK-Cu: Genomic Modulation and Extracellular Matrix Architecture
Glycyl-L-histidyl-L-lysine (GHK) is a naturally occurring tripeptide found in high concentrations within human plasma, saliva, and urine. The peptide is defined by its incredibly strong binding affinity for copper ions, spontaneously forming the GHK-Cu complex upon exposure to copper in the physiological environment. Baseline levels of GHK-Cu in the human body peak at roughly 200 ng/mL during late adolescence (around age 20), but suffer a precipitous and permanent decline as an individual ages, dropping to approximately 80 ng/mL by age 60. Gerontological researchers heavily correlate this severe drop in systemic GHK-Cu concentrations with the parallel, systemic decline in human regenerative capacity, skin elasticity, and delayed wound healing observed in elderly populations.
Unlike standard signaling peptides that trigger a single cascading pathway, GHK-Cu operates as a profound genomic modulator. Exhaustive genetic profiling studies utilizing the Broad Institute Connectivity Map indicate that the GHK-Cu molecule can actively upregulate or downregulate the expression of over 4,000 distinct human genes. This massive genomic influence allows the peptide to effectively reset pathological, age-degraded gene expression patterns back to a healthier, more youthful state of cellular function. Among its most well-documented and heavily utilized aesthetic effects are the aggressive stimulation of collagen, elastin, and glycosaminoglycan synthesis. GHK-Cu physically rebuilds the extracellular matrix, restoring structural integrity to dermal and connective tissues, thereby reversing skin thinning, increasing dermal density, and eliminating fine lines.
Furthermore, GHK-Cu exerts incredibly potent systemic anti-inflammatory effects by aggressively suppressing pro-inflammatory cytokines such as TNF-α, IL-6, and IL-1β. Recent, highly detailed systemic studies focusing on murine models of dextran sulfate sodium (DSS)-induced ulcerative colitis have elucidated the specific genetic mechanisms driving GHK-Cu’s anti-inflammatory power. The research reveals that GHK-Cu modulates the NAD-dependent deacetylase sirtuin-1 (SIRT1) and the signal transducer and activator of transcription 3 (STAT3) signaling pathway. The STAT3 pathway, when improperly regulated, amplifies inflammatory cascade reactions by upregulating key genes responsible for Th17 cell differentiation, a primary driver of tissue damage in inflammatory bowel disease. By upregulating and activating SIRT1, which subsequently deacetylates and functionally inhibits STAT3, GHK-Cu entirely short-circuits the inflammatory cascade, promotes profound mucosal healing, and restores the integrity of tight junction proteins (such as ZO-1 and Occludin) within the cellular barrier.
The Synergistic Hypothesis: Deconstructing the Glow Blend
The KLIKGLOW formulation utilizes a specific, deliberately calibrated mass ratio of 5:1:1 (50mg GHK-Cu, 10mg BPC-157, 10mg TB-500). To fully appreciate the clinical intention behind this formulation, one must analyze the history of peptide stacking. In clinical sports medicine and underground biohacking contexts, the combination of merely BPC-157 and TB-500 has long been referred to as the “Wolverine Stack”—named after the comic book character known for instantaneous cellular regeneration. This duo is celebrated for its capacity to address deep musculoskeletal trauma from both localized (BPC-157) and systemic (TB-500) vectors. The addition of 50mg of GHK-Cu elevates this aggressive repair protocol into a “Hyper Recovery Stack” or “Glow Fusion,” specifically engineering the blend to support massive cosmetic, aesthetic, and structural regeneration alongside the deep-tissue healing provided by the Wolverine base.
The underlying pharmacological rationale for this specific tripartite combination relies on targeting multiple physiological bottlenecks simultaneously, thereby preventing the biological healing process from stalling at any single point of failure.
Table 1: Synergistic Functional Distribution of the KLIKGLOW Protocol
| Constituent Peptide |
Molecular Role in the Blend |
Primary Mechanism of Action |
Clinical Synergy and Outcome |
| BPC-157 (10mg) |
Environmental Conditioning |
Upregulates VEGFR2, modulates Nitric Oxide, and suppresses localized acute inflammation. |
Optimizes the biochemical environment, ensuring massive blood flow and oxygenation to the injury site, prepping the area for structural repair. |
| TB-500 (10mg) |
Cellular Migration Logistics |
Sequesters G-actin, regulates cytoskeletal dynamics, and heavily enhances progenitor cell mobility. |
Drives the physical movement of necessary repair cells into the highly optimized environment created by BPC-157, ensuring rapid biological action. |
| GHK-Cu (50mg) |
Structural Matrix Architecture |
Modulates gene expression across 4000+ genes, forces collagen/elastin synthesis, acts as an antioxidant. |
Rebuilds the extracellular matrix using the resources provided by the other peptides, preventing fibrotic scarring, restoring elasticity, and ensuring the long-term physical durability of the newly repaired tissue. |
Clinical researchers utilizing peptide therapies note that when administered in isolation, a single peptide may successfully upregulate a specific biological pathway, only to have the overall healing process hindered by a secondary biological limitation.
For instance, BPC-157 may successfully optimize local blood flow to a torn ligament, but without the aggressive actin-regulating properties of TB-500, cellular migration to that ligament may remain sluggish. Conversely, both peptides may heal the ligament rapidly, but without the collagen-organizing power of GHK-Cu, the resulting repair may be structurally weak or plagued by rigid, fibrotic scar tissue.
By deploying these three compounds synergistically, the KLIKGLOW blend attempts to construct a flawless, uninterrupted, multi-pronged biological pipeline for absolute tissue regeneration.
However, the stacking of highly active experimental peptides is not universally endorsed within the medical community. Conservative clinicians frequently warn against “kitchen sink” pharmacology—the practice of combining numerous experimental compounds without understanding their complex interactions. The primary clinical concern with stacks like the Glow Blend is signal degradation and redundancy. When multiple compounds heavily stimulate angiogenesis and cellular migration simultaneously, the physiological “signal quality” can become chaotic. If a patient improves rapidly, or conversely, suffers a severe adverse reaction, the presence of multiple unapproved compounds makes it biologically impossible to isolate which specific peptide was responsible for the outcome, rendering the treatment scientifically unmonitorable.
The Reality of Human Clinical Trials: Status and Safety Data
Despite the immense commercial popularity, the multimillion-dollar grey market economy, and the incredibly robust body of preclinical animal data demonstrating miraculous healing properties, the landscape of rigorous, large-scale, placebo-controlled human clinical trials for these specific peptides remains extraordinarily sparse. Regulatory bodies globally continue to emphasize that, as of 2026, none of the specific formulations contained within the KLIKGLOW complex have achieved standard medical approval for human therapeutic use. The disparity between in-vitro success and human clinical validation remains the most significant barrier to the mainstream adoption of peptide therapies.
BPC-157: Clinical Stagnation and Theoretical Oncological Risks
To date, BPC-157 remains categorized as an experimental, unapproved substance with virtually no high-quality, peer-reviewed, randomized controlled trials (RCTs) demonstrating definitive safety and efficacy in human populations. The clinical history of BPC-157 is defined by abandoned research and unpublished data.
A formal Phase I clinical trial assessing the basic safety and pharmacokinetics of BPC-157 (then operating under the developmental name Bepecin, sponsored by PharmaCotherapia) was initiated in 2015 (ClinicalTrials.gov Identifier: NCT02637284). The trial recruited 42 healthy volunteers (aged 18-35) to receive single and multiple oral doses. However, the study was abruptly cancelled by the researchers in 2016, and the data and results were never submitted or published in any peer-reviewed format. The exact reasons for this cancellation remain undisclosed, leaving a massive void in baseline human safety data.
Additionally, various scientific abstracts frequently reference an early Phase II trial utilizing BPC-157 for ulcerative colitis, heavily claiming a “very safe profile” devoid of toxic effects; however, comprehensive, long-term, peer-reviewed data for this trial remains conspicuously absent from the scientific literature, leading researchers to treat such claims with extreme skepticism.
Recent years have yielded only minor, highly localized pilot data. A small 2024/2025 pilot study evaluated the acute intravenous infusion of BPC-157 (dosed at 10mg followed by 20mg the next day) in merely two healthy human adults. The limited results indicated no measurable adverse acute effects on hepatic, renal, cardiac, or thyroid biomarkers, suggesting basic short-term tolerability. Another highly cited, but poorly designed, small retrospective study evaluated 12 patients who received intra-articular injections of BPC-157 for chronic, unspecified knee pain; while 7 of the 12 patients reported subjective pain relief exceeding six months, the complete absence of a placebo control group or standardized pain-scale methodology severely limits the scientific validity and reproducibility of the findings.
The absolute lack of long-term human safety data is critically concerning due to BPC-157’s primary mechanism of action. Because the peptide potently and aggressively stimulates angiogenesis via the VEGF/VEGFR2 pathways, there is a theoretical, but highly biologically plausible, risk that BPC-157 could inadvertently supply massive new blood flow to existing, undiagnosed malignant tumors, thereby acting as a catalyst for rapid cancer metastasis.
The VEGF/VEGFR2 pathways are known to be highly active in roughly half of all human cancers, ranging from ovarian cancer to melanoma. While a highly isolated 2004 laboratory study reported that BPC-157 inhibited the growth of a specific melanoma cell line in a petri dish, more recent animal experiments utilizing mice implanted with active cancer cells found that the administration of BPC-157 did not meaningfully shrink the tumors. The mixed signals regarding the peptide’s interaction with malignant cells lead regulatory scientists to unequivocally conclude that BPC-157 poses an unacceptable risk to individuals with active or suspected malignancies, as introducing a potent growth-promoting angiogenesis catalyst into an oncological environment could be catastrophic.
TB-500: The Diagnostic Discrepancy of the Fragment
An accurate clinical analysis of TB-500 requires a strict, uncompromising differentiation between the synthetic heptapeptide fragment (TB-500) and the naturally occurring, full-length 43-amino-acid parent protein (Thymosin Beta-4, or Tβ4). The failure to distinguish between these two molecules is the primary source of misinformation surrounding TB-500’s safety profile.
The parent molecule, Thymosin Beta-4, has undergone various legitimate Phase I and Phase II clinical trials with highly encouraging results. A Phase I safety trial evaluating the administration of synthetic Tβ4 at massive doses ranging from 42mg to 1260mg over 14 days demonstrated excellent tolerability with no severe toxicities or serious adverse events reported in healthy adults. Furthermore, targeted ophthalmic trials utilizing Tβ4-based eye drops (such as the RGN-259 formulation) have demonstrated safety and clinical efficacy in treating severe dry eye conditions, bacterial corneal infections, and physical corneal wounds. Preliminary cardiac studies have also explored the use of recombinant human Tβ4 following severe ST-segment elevation myocardial infarctions (STEMI), with early pilot data suggesting the intervention is feasible, safe, and potentially capable of improving left ventricular ejection fractions by more than 50% in specific cohorts six months post-infarction.
Conversely, the synthetic, seven-amino-acid fragment known specifically as TB-500 (Ac-LKKTETQ)—the exact peptide utilized in the KLIKGLOW formulation—has absolutely zero completed Phase II or Phase III human clinical trials verifying its safety or efficacy for musculoskeletal repair. Currently, only one highly conceptual, fictionalized Phase 1/2 study (NCT07487363) exists in trial registries as a placeholder example for evaluating TB-500 in patients with stable atherosclerotic cardiovascular disease, further highlighting the absolute lack of real-world human data for the fragment.
Much of the commercial marketing for gray-market TB-500 aggressively conflates the verified clinical success of the full-length parent molecule with the untested synthetic fragment. Consequently, long-term human safety data, optimal dosing parameters, and known contraindications for the specific Ac-LKKTETQ fragment remain entirely non-existent.
Like BPC-157, TB-500 possesses potent pro-angiogenic properties; therefore, researchers warn that it carries the identical theoretical risk of exacerbating oncological conditions by promoting new blood vessel formation within tumor microenvironments, rendering it unsafe for use in patients with a history of cancer. Furthermore, a 2024 pharmacological study revealed a startling finding: the TB-500 sequence (Ac-LKKTETQ) itself did not actually increase wound-healing activity in vitro. Instead, the researchers found that one of its metabolic breakdown products—the smaller fragment Ac-LKKTE—was responsible for the biological activity, suggesting that the entire pharmacological understanding of how TB-500 operates may be flawed or incomplete.
GHK-Cu: Topical Supremacy vs. Injectable Toxicity Risks
The clinical safety profile and therapeutic viability of GHK-Cu are inextricably linked to, and highly dependent upon, its specific route of administration. When administered topically, GHK-Cu enjoys a decades-long history of exceptional safety and profound efficacy within the mainstream cosmetic and dermatological industries. Extensive clinical testing has verified that the topical application of GHK-Cu serums and creams successfully increases dermal thickness, reduces skin laxity, accelerates epithelialization, and minimizes fine lines and photodamage without initiating any adverse systemic toxicity. Because topical absorption limits the systemic penetration of the copper ion, the risk profile is considered exceptionally low, leading the compound to be described by researchers as a safe, inexpensive, and extensively studied aesthetic therapeutic.
However, the KLIKGLOW 70mg formulation is explicitly designed for reconstitution and subsequent subcutaneous or intravenous injection, forcefully introducing the compound directly into the systemic circulation. Systemic human safety trials for injectable GHK-Cu are severely lacking, and the transition from topical cosmetic to systemic biologic introduces massive pharmacological variables.
The primary clinical concern associated with the systemic injection of GHK-Cu is the forced introduction of exogenous copper directly into the bloodstream. While copper is an essential trace mineral required for iron metabolism and neurotransmission, excessive systemic accumulation carries a very real risk of acute copper toxicity. The clinical symptoms of copper toxicity are severe and include severe abdominal pain, persistent vomiting, uncontrollable tremors, fever, anemia, and distinct metallic tastes. While researchers note that the LD50 (lethal dose) for GHK-Cu in murine models equates to an impossibly massive single dose of roughly 23,000mg for a 70kg human adult—rendering acute lethal toxicity highly improbable at the standard aesthetic therapeutic doses of 5-50mg—the long-term cumulative effects of daily copper peptide injections remain entirely unmapped in human populations.
Injectable applications demand strict consideration of the patient’s total systemic copper load, making the compound absolutely contraindicated for individuals suffering from genetic conditions affecting copper metabolism, such as Wilson’s disease or Menkes disease. Furthermore, the United States Food and Drug Administration (FDA) has explicitly and formally warned that compounded injectable drugs containing GHK-Cu present significant risks for severe immunogenicity. The agency notes that the peptide is highly susceptible to protein aggregation and the accumulation of peptide-related manufacturing impurities when formulated for injection, which can trigger massive, systemic immune system reactions in human patients.
Table 2: Clinical Trial Status and Primary Safety Concerns of the KLIKGLOW Components
| Compound |
Completed Phase II/III Human Trials |
Primary Form of Evidence |
Critical Safety Warnings and Contraindications |
| BPC-157 |
Zero. Phase I trial (NCT02637284) aborted in 2016 without data publication. |
Rodent models, in-vitro tissue repair assays, anecdotal case reports. |
Theoretical pro-tumorigenic risk due to VEGFR2 angiogenesis. Contraindicated in suspected malignancies. |
| TB-500 |
Zero. (Parent molecule Tβ4 has completed trials; synthetic fragment Ac-LKKTETQ has none). |
Extrapolation from full-length Tβ4 trials, equine/veterinary studies. |
Potential promotion of tumor vasculature. Long-term toxicity and optimal human dosing completely unknown. |
| GHK-Cu (Injectable) |
Zero for Injectable Formats. (Extensive trials for topical cosmetic applications). |
Decades of topical dermatological data; genomic profiling maps. |
Risk of systemic copper toxicity; severe immunogenicity risks from peptide aggregation; site injection pain. |
Real-World Utilization: Social Media Ethnography and Patient Outcomes
Because rigorous, peer-reviewed clinical data regarding the systemic use of this specific tri-peptide stack is virtually non-existent, the vast majority of the prevailing human efficacy and safety data is entirely anecdotal. This data is driven almost exclusively by the explosive, uncontrolled growth of the biohacking, longevity, and experimental aesthetics communities operating on social media platforms such as TikTok, Reddit, and specialized Telegram channels. Influencers, combat athletes, and aggressive longevity optimization clinics routinely market this peptide combination to millions of consumers, effectively bypassing traditional, conservative medical frameworks and initiating a massive, uncontrolled human trial. A rigorous ethnographic analysis of these digital communities (particularly deep-dive forums such as Reddit’s r/Peptides and r/crossfit) reveals a complex dichotomy of miraculous physiological benefits juxtaposed against terrifying, long-lasting adverse events.
Observational Efficacy Reports
Users self-administering the KLIKGLOW components (or identical 5:1:1 ratios of GHK-Cu, BPC-157, and TB-500) report remarkable physiological benefits that closely align with the theoretical mechanisms outlined in preclinical animal data. In the realm of musculoskeletal recovery, athletes and individuals suffering from chronic pain document the rapid, almost instantaneous resolution of chronic tendinopathies, the accelerated healing of acute muscle tears, and significant, systemic reductions in joint inflammation. Users frequently note that injuries that remained stagnant after months of traditional physical therapy resolved within weeks of initiating the peptide protocol.
Aesthetically, users utilizing the tri-peptide stack heavily report profound improvements in skin hydration, dermal firmness, and the rapid clearing of traumatic bruising. In one highly detailed Reddit case report, a female user documented that her chronic bruising, which typically lasted weeks, resolved in a mere 3-4 days after initiating the GHK-Cu/BPC-157/TB-500 stack.
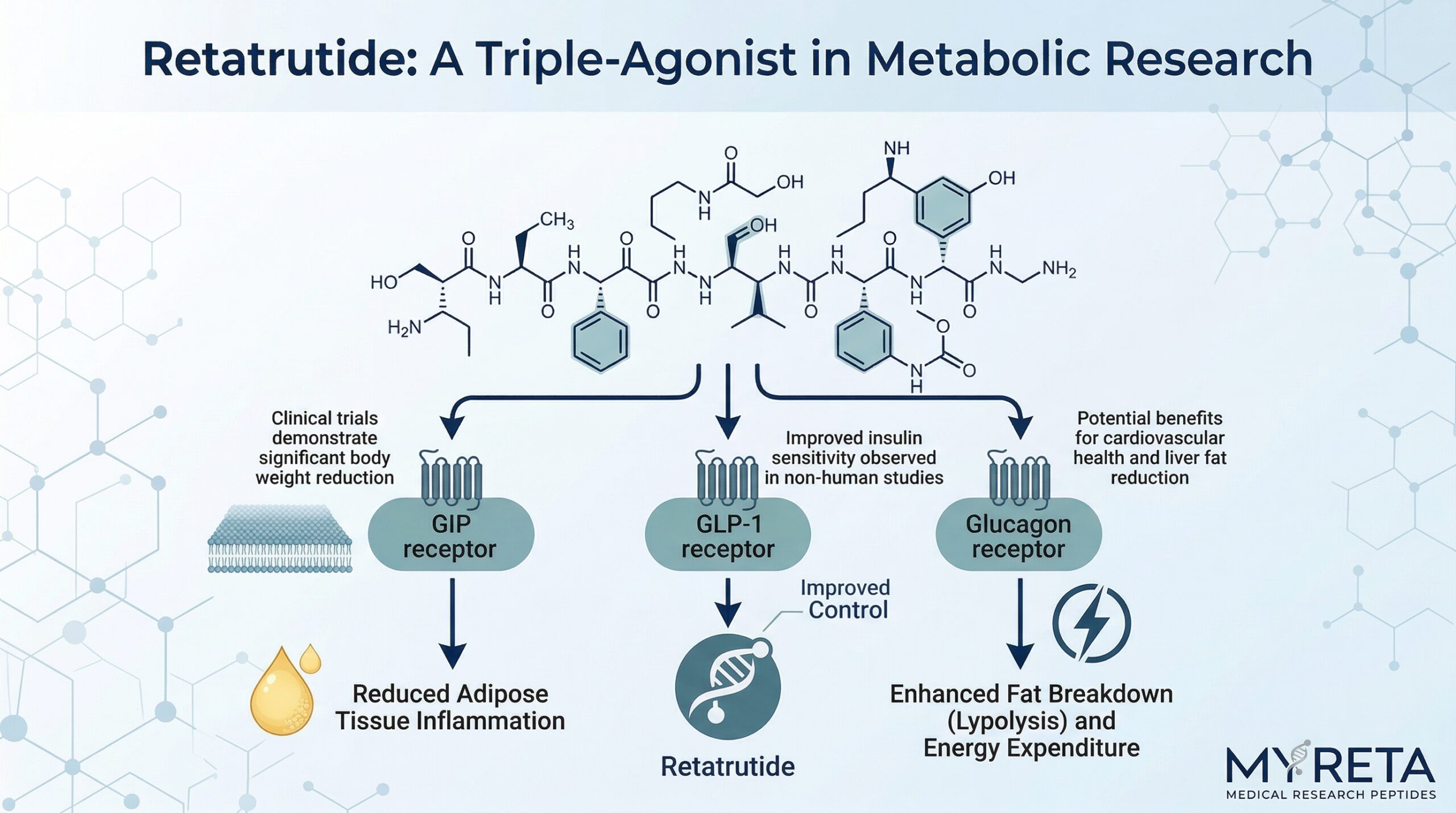
Furthermore, this same user reported unexpected, robust regrowth of fine hair. She noted that her hair had thinned severely due to a compounding history of Anavar (a DHT-derivative steroid) usage, acute autoimmune thyroiditis, and rapid weight loss induced by the GLP-1 receptor agonist retatrutide. After three weeks of utilizing the peptide stack, she observed massive “baby hair” sprouting and noticeably increased volume at the scalp level, a finding she corroborated with numerous other users reporting “hard to believe” amounts of hair growth linked specifically to systemic GHK-Cu administration.
Observational Adverse Events and Severe Toxicities
Conversely, the unregulated, experimental nature of this digital ecosystem has brought significant, highly concerning adverse effects to light, severely underscoring the dangers of self-administering experimental systemic therapeutics.
The most universal complaint regarding the protocol is extreme injection site pain. The subcutaneous injection of GHK-Cu is notoriously associated with localized tissue distress, often referred to colloquially as the “copper uglies”. Users frequently report significant stinging upon injection, followed by prolonged tissue tenderness, extreme localized redness, and aggressive swelling. Many users in these forums attribute this reaction to acute mast cell activation triggered by the peptide complex, noting that they require the concurrent, daily use of potent systemic antihistamines (such as Xyzal) simply to tolerate the basic administration of the protocol.
Beyond localized pain, rare but severe adverse reports highlight the potential for systemic immunological and psychiatric distress. One user documented a harrowing experience wherein a mere nine-day cycle of a low dose (60 micrograms) of BPC-157 triggered a massive, acute autoimmune-like systemic reaction. The user reported that their body began “attacking its own joints,” resulting in debilitating pain, an inability to walk or stand, and severe gastrointestinal cramping. Most terrifyingly, this autoimmune crash was accompanied by profound psychiatric collapse.
The user reported developing severe, unrelenting anhedonia (the total inability to feel pleasure), crippling anxiety, and a pervasive sense of “gloom and doom”. Despite only utilizing the peptide for nine days, the user reported that these debilitating physical and psychiatric side effects persisted for an astonishing 11 months.
Given BPC-157’s scientifically documented, complex interactions with the dopaminergic and serotonergic systems in rat models—specifically its ability to modulate dopamine release and mitigate serotonin syndrome—it is highly pharmacologically plausible that the exogenous introduction of BPC-157 can induce profound, long-lasting disruptions in central nervous system neurotransmitter balance in susceptible human individuals. These ethnographic reports serve as a chilling reminder that manipulating master regulatory pathways without clinical oversight carries massive, potentially permanent neurological risks.
The 2026 Regulatory Landscape: FDA Volatility and Global Enforcement
The regulatory status of therapeutic peptides in early 2026 is characterized by extreme legal volatility, unprecedented political intervention, and widespread market confusion spanning across global regulatory bodies, including the US Food and Drug Administration (FDA), the UK Medicines and Healthcare products Regulatory Agency (MHRA), and the World Anti-Doping Agency (WADA). The classification of the KLIKGLOW components is currently the subject of intense legal and political warfare.
FDA Categorization and the 2026 RFK Jr. Reclassification Announcement
To understand the current legal status of these compounds in the United States, one must examine the actions taken by the FDA under Sections 503A and 503B of the Federal Food, Drug, and Cosmetic Act, which govern the practice of pharmaceutical compounding.
In late 2023, the FDA aggressively updated its bulk drug substances list. Citing significant, unresolved safety risks, a total lack of robust human clinical efficacy data, and grave concerns over immunogenicity and peptide-related impurities, the FDA officially designated 19 of the most popular therapeutic peptides—explicitly including BPC-157, TB-500 (Thymosin beta-4 fragment), and injectable GHK-Cu—as “Category 2” bulk drug substances. This Category 2 designation was a devastating blow to the clinical peptide industry. It formally identified these compounds as presenting potential safety risks and rendered them entirely ineligible for routine compounding. The ruling effectively banned licensed U.S. compounding pharmacies from legally preparing or dispensing BPC-157, TB-500, or injectable GHK-Cu, even with a valid physician’s prescription.
This prohibition forced millions of patients who relied on these therapies for chronic pain and autoimmune management out of the safe, regulated medical system, driving them directly into the arms of unregulated, highly dangerous overseas gray-market “research chemical” suppliers.
However, the regulatory paradigm experienced a massive, unprecedented political shockwave in early 2026. On February 27, 2026, the newly appointed Department of Health and Human Services (HHS) Secretary, Robert F. Kennedy Jr., made a highly publicized appearance on The Joe Rogan Experience podcast. During the broadcast, Secretary Kennedy fiercely criticized the FDA’s 2023 peptide ban as regulatory overreach, arguing that the agency lacked the required safety signals to justify the draconian restrictions. Kennedy explicitly announced his intention to override the FDA, stating that approximately 14 of the 19 restricted peptides—specifically targeting BPC-157, TB-500, and GHK-Cu—would be formally removed from the Category 2 restriction list and moved back to Category 1 status within “a couple of weeks”.
Returning these compounds to Category 1 status would instantly restore legal access, allowing licensed 503A compounding pharmacies to once again synthesize and dispense these peptides to patients under strict physician supervision, thereby crushing the dangerous black market.
Despite the massive surge in public excitement and the celebratory press releases issued by wellness clinics following the HHS Secretary’s podcast announcement, specialized regulatory attorneys and legal experts have issued stark, sobering warnings to the medical community. As of April 2026, the legal reality does not match the political rhetoric. No formal Federal Register notice has been published, and no official FDA regulatory rule has been amended to enact this promised reclassification. Legal experts stress that public statements made on a podcast do not constitute binding regulatory action; therefore, compounding BPC-157, TB-500, or injectable GHK-Cu currently remains a violation of federal law.
Furthermore, legal analysts emphasize a critical, often misunderstood distinction: returning a peptide to Category 1 compounding eligibility is absolutely not the equivalent of achieving FDA drug approval. Even if reclassified, these peptides will remain unapproved, investigational, off-label therapeutics lacking formal Phase III clinical trials, and they will never be available over-the-counter.
Table 3: Summary of the 2026 U.S. FDA Regulatory Status for the KLIKGLOW Components
| Peptide Compound |
FDA 503A/503B Status (As of April 2026) |
Primary FDA Safety Rationale for Restriction |
Expected Action per HHS Secretary RFK Jr. (Feb 2026) |
| BPC-157 |
Category 2 (Restricted) |
Immunogenicity risks; complexities in API characterization; lack of human safety data. |
Expected return to Category 1 (Legal for Compounding). |
| TB-500 |
Category 2 (Restricted) |
Lack of human exposure data; unmapped toxicity and pro-tumorigenic potential. |
Expected return to Category 1 (Legal for Compounding). |
| GHK-Cu (Injectable) |
Category 2 (Restricted) |
High risk of peptide aggregation and manufacturing impurities leading to systemic immune reactions. |
Expected return to Category 1 (Legal for Compounding). |
UK MHRA Enforcement and the Research Loophole
In the United Kingdom, the Medicines and Healthcare products Regulatory Agency (MHRA) has adopted an increasingly strict, combative posture toward the surging peptide gray market. From a purely criminal standpoint, products like BPC-157, TB-500, and GHK-Cu are not classified as controlled substances under the Misuse of Drugs Act 1971; therefore, mere possession of the KLIKGLOW complex by an individual is not an inherently criminal offense. They are legally imported, bought, and sold under the strict caveat that they are “research chemicals” expressly not intended for human consumption.
However, this massive gray-market loophole has allowed an explosion of underground wellness clinics, cosmetic spas, and fitness influencers to actively, and illegally, market these unregulated injectables for therapeutic use. The MHRA has forcefully intervened, explicitly stating that any clinic or digital vendor making medicinal claims regarding these peptides—such as claiming BPC-157 “aids in tissue repair” or GHK-Cu “reverses aging”—is in direct, flagrant breach of the Human Medicines Regulations 2012.
In response to the rapidly growing public health crisis of thousands of citizens self-injecting completely unregulated, potentially contaminated products, the MHRA has initiated widespread investigations into aesthetic clinics and has executed coordinated raids on illicit manufacturing facilities suspected of synthesizing illegal peptide medications.
WADA Prohibitions in Competitive Sports
For competitive athletes navigating this complex landscape, the regulatory stance is entirely unambiguous and brutally strict. The World Anti-Doping Agency (WADA) has universally prohibited the use of both BPC-157 and TB-500 at all times, both in and out of competition. BPC-157 falls under the “S0 Unapproved Substances” category, a blanket ban covering any pharmacological substance not currently approved by any governmental regulatory health authority for human therapeutic use. TB-500 is specifically categorized under the “S2 Peptide Hormones, Growth Factors, Related Substances, and Mimetics” classification, strictly banning its use due to its performance-enhancing effects on tissue regeneration and cellular mobility. Consequently, any use of the KLIKGLOW blend by tested, competitive athletes carries severe compliance risks, guaranteeing immediate doping infractions and potential career-ending bans.
Conclusion: The Edge of Experimental Medicine
The KLIKGLOW (BPC-157, TB-500, GHK-Cu) 70mg formulation represents the absolute bleeding edge of experimental, combinatorial regenerative medicine. Pharmacologically, the specific 5:1:1 combination provides a highly coherent, theoretically flawless, synergistic approach to complete tissue repair. By deploying BPC-157 to optimize the vascular environment and eliminate inflammation, utilizing TB-500 to vastly accelerate the logistical migration of repair cells, and leveraging the massive genomic modulating power of GHK-Cu to rebuild the structural extracellular matrix, the protocol attempts to eliminate every biological bottleneck associated with healing and aging.
From a regulatory standpoint, the landscape in early 2026 is defined by unprecedented political chaos and legal instability. While the HHS Secretary’s aggressive recent announcement strongly signals an imminent return to legal, regulated 503A compounding for these substances in the United States—which would drastically improve product safety and purity—they currently remain illegal to compound, investigational, and totally unapproved. Until global regulatory bodies formalize these political reclassifications, and until rigorous, Phase III clinical trials establish irrefutable, standardized safety and dosing protocols, the systemic utilization of complex, multi-peptide formulations like the KLIKGLOW 70mg complex remains a scientifically brilliant, yet inherently hazardous, clinical endeavor.